Actualizat: 18-03-2025 / Publicat: 27-10-2020
.jpg)
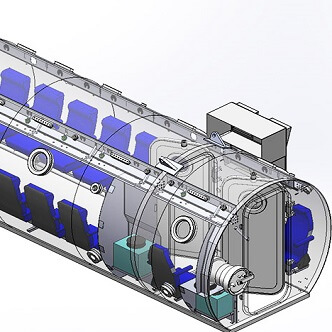
Discover the hyperbaric medicine center opened in our clinic. Centrokinetic has the top-performing hyperbaric chamber in Bucharest, with multiple medical and anti-aging uses. The Baroks chamber has 5 seats, and operates at a constant pressure of 2.5 atmospheres, being fully automated and having protocols for each condition, and can be used individually for each patient.
Hyperbaric oxygen therapy - benefits
Patients who use the clinic's hyperbaric therapy services benefit from:
- The only medically accredited hyperbaric therapy chamber in Bucharest, which operates at 2.5 atmospheres (those for aesthetic use go to 1 atmosphere and have no medical benefits).
- A safe medical procedure, without irradiation, without pain, without other side effects.
- The specialized medical team consists of recovery doctors, orthopedists, rheumatologists, neurologists, and neurosurgeons, meaning a multidisciplinary team specialized in all diseases that can be treated with hyperbaric therapy.
- Premium conditions at a fair price. Our clinic is recognized for the conditions offered and for the care of each patient. But we do not need to pay exorbitant prices to have access to quality medical services. At Centrokinetic you can find an affordable and fair price. But note that we do not have a contract with the National Health Insurance House (we do not offer state reimbursed services)
Centrokinetic is keeping contact with prestigious clinics and universities in Belgium, the Netherlands, France, and Greece to constantly update treatments to provide patients with the best medical solutions.
What is femoral head necrosis?
Femoral head necrosis (FHN) is a condition caused by poor circulation in the subchondral bone. Although the etiology of this disease is not yet fully understood, there are several traumatic and atraumatic factors that are associated with the disease. The pathophysiology of the disease is characterized by the death of bone marrow and osteocytes. If left untreated, the disease can progress to bone collapse, and thus the development of osteoarthritis.
While the early stages of the disease are asymptomatic, it is possible to painfully limit active and passive hip movement. Currently, an optimal treatment protocol for FHN cannot be identified. Post-collapse cases require surgery, basic decompression, or total hip arthroplasty. However, current progress is being made in conservative management. One of the possible conservative ways that can effectively delay hip arthroplasty or prevent the need for a surgical approach is hyperbaric oxygen therapy (HBO). HBO increases extracellular oxygen concentration and reduces ischemia and cellular edema by inducing vasoconstriction. Studies have reported radiographic improvements, reduced pain and increased range of motion for the early stages of the disease.
Introduction
Femoral head necrosis (FHN), also called avascular necrosis, or femoral head osteonecrosis is a common multifactorial condition that affects patients of any age and can lead to substantial clinical morbidity. Osteonecrosis is characterized by a lack or insufficiency of blood flow to bone tissue and leads to the death of osteocytes and bone marrow.
As reported by Parsons and colleagues, it most commonly occurs at the age of 25 or between the ages of 20 and 30 in men. Epidemiology reveals between 10,000 and 20,000 new cases of FHN diagnosed each year in the United States. In Western countries, the prevalence of the disease is at an average age of 39 years, and 10% of the hip replacements performed are due to FHN. The collapse of the femoral head, degenerative lesions of the hip joint, and subsequent long-term disability are possible adverse consequences of untreated or undiagnosed FHN. In particular, it is estimated that more than 70% of femoral heads with osteonecrosis will continue to deteriorate, requiring replacement of the prosthetic joint within 3-4 years of diagnosis. The disease is responsible for 5-18% of all hip replacements performed. Moreover, similar pathophysiology may occur in other joint areas (eg, femoral condyle, wrist, humerus head, and distal talus) caused by comparable avascular syndromes. Multifocal osteonecrosis is defined as a disease involving three or more anatomical areas separated simultaneously or consecutively.
Hyperbaric oxygen treatment
Hyperbaric oxygen therapy (HBO) is one of the proposed treatments. Indeed, tissue oxygen promotes angiogenesis that reduces edema. Moreover, by reducing intravenous pressure, venous drainage is restored and microcirculation is improved. Restricted to the considered stage, Camporesi and collab. showed that HBO should be considered the primary treatment modality in any patient and especially in young patients, where the goal is to delay the total arthroplasty of the hip as long as possible. Therefore, the European Community accepted femoral head necrosis as an indication for hyperbaric oxygen therapy (HBOT) during the Consensus Conference in Lille, France.
Initially, the relationship between femoral head necrosis and HBOT was thoroughly analyzed in a specific chapter published in Hyperbaric Medicine Practice. Camporesi reported accurate diagrams of patient outcomes and a detailed review of the literature up to 1997, as well as various pathological outcomes and justification for treatment. Recently, Bosco and colleagues proposed an extensive report on this topic. They accurately updated the scientific literature until 2016 and summarized, for the eligibility of the paper for the study, the number of patients, the target, and the results obtained. Although management, care, and treatment options are clearly mentioned for pathology, the available results differ from each other depending on the stratification criteria and the particular stage of the disorder. This chapter aims to review more recent evidence from the scientific literature, presenting the physiology and current state of pathology and therapy for femoral head necrosis. In particular, we focused on therapeutic mechanisms of action with hyperbaric oxygen (HBO) for femoral head necrosis.
 | .jpg) |
Etiology
In the FHN study, the absence of a model on bipedal mammals limits our knowledge of risk factors and disease pathogenesis. Also, completing long-term studies is difficult for researchers and clinicians. However, the scientific community agrees that ischemia plays a major role in pathogenesis. As mentioned above, FHN is a multifactorial disease in which both genetic and daily life factors lead to pathology. When evaluating patients with osteonecrosis, physicians should first differentiate between primary ("idiopathic") osteonecrosis and secondary osteonecrosis. Although the etiology of secondary osteonecrosis has not been delineated, risk factors include both traumatic and non-traumatic conditions (ie, corticosteroid use, alcohol consumption, smoking, coagulation abnormalities, etc.).
Traumatic events can lead to bone fractures or, in the worst case, to the displacement of the femoral head; since trauma occurs, it leads directly to the interruption of the femoral head's blood supply. Malizos and colleagues distinguished different pathogenesis in patients with sub-capital fracture and patients with hip dislocation. In the first case, 10–20% of the vascularization of the femoral head is preserved from the ligament. Instead, as the hip dislocates, the blood supply is interrupted, and the infusion depends on the integrity of the retinacular vessels.
Otherwise, non-traumatic osteonecrosis is frequently associated with pathologies in which treatment with corticosteroids is necessary (ie systemic lupus erythematosus, organ transplantation, lymphoma, etc.). A report described the case of a woman who was only 18 years old when she underwent surgery due to bilateral osteonecrosis of the femoral condyles that developed during the treatment of a hematological malignancy. Even if the scientific literature does not know the exact dose of steroids needed to induce osteonecrosis, the higher the dose, the greater the risk. Indeed, the average daily or maximum dose took seems to be more involved than the cumulation or duration of therapy. Also, alcohol dependence is a risk factor for FHN.
In comparing the gender difference, studies indicated for men a higher frequency of alcohol-induced FHN compared to women. Indeed, Shimizu and colleagues have shown a greater susceptibility of men to developing FHN in response to alcohol consumption. Specifically, women did not develop osteonecrosis for alcohol consumption for both short and long periods. However, further investigations are needed among the sex factors responsible for this evidence.
Additional risk factors for FHN can be identified in bone marrow transplantation, as well as meta-static malignancies and pregnancy. Also, they can be associated with pathologies such as hyperuricemia, pancreatitis, and leukemia or lymphoma.
Pathophysiology
The pathophysiology of FHN is characterized by a complex series of events that lead to cell death and osteogenic processes. The pathogenic course begins with two associated mechanisms: interstitial bone marrow edema and necrosis of hematopoietic cells and adipocytes. Histological signs appear almost 24–72 hours after anoxia, even if osteocyte necrosis is evident after about 2-3 hours of lack of oxygen. These stimuli induce bone remodeling processes. Initially, inflammatory signs (i.e, reactive hyperemia, and capillary revascularization) surround the necrotic area. Thus, this mechanism initiates bone repair in which the new bone struggles to remove and replace dead tissue.
However, bone remodeling is inefficient due to dead trabeculae, where new bone is placed. Moreover, osteolysis goes beyond osteogenesis and this leads to loss of structural integrity of the trabeculae, with subchondral fracture and joint incongruence. Altered subchondral vascularity is the underlying pathophysiological sign for FHN. Kiaer and colleagues indicated that a 60% drop in blood intake will lead to a decrease in pO2 from 75 mmHg to 50 mmHg. Consequently, it will cause obvious ischemia.
Different pathogenic mechanisms can lead to FHN. Cytotoxicity due to radiation exposure, chemotherapy or thermal damage causes direct death of bone marrow cells and osteocytes, although this has not yet been shown in vivo. Also, three main pathogenic mechanisms can lead to ischemic disorders and subsequent femoral head necrosis:
- Vascular disruption due to fractures or dislocation (i.e traumatic osteonecrosis). Femoral fractures or hip displacement usually cause extra-bone arterial involvement. Specifically, when the fracture occurs inside the joint capsule, the vessels that oxygenate the subchondral bone suffer a direct trauma. A relatively high incidence of FHN has been reported in patients with these fractures.
- Intravascular coagulation and microcirculatory thrombosis. Different pathways can lead to the same vascular obstructions which mean sickle cell aggregations, clots, or lipid thrombi. Thrombotic emboli can occur both in the arteries and venous areas, in samples of osteonecrosis tissue; In some animal models, they have been associated with osteocyte necrosis. The prevalence of osteonecrosis induced by sickle cell anemia is between 37 and 50%. The weak arterial network of the hip joint facilitates vascular occlusion by diseased cells. In these patients, low-oxygen environments are thought to trigger hemoglobin precipitation leading to erythrocytes. More than that, the complication rate for patients with affected cells following orthopedic procedures is significantly higher than for healthy patients. Consequently, early and alternative interventions are critical to successfully delay total hip arthroplasty.
Coagulation disorders are also involved in FHN. For example, genetic defects resulting from hypofibrinolysis or thrombophilia can lead to increased thrombus formation and obstruction of blood flow to bone tissues. However, using a case study methodology, high levels of coagulation factors have been reported in patients with osteonecrosis showing the absence of known genetic defects. Jarman and colleagues have shown that osteonecrosis caused by coagulation abnormalities is aggravated by testosterone therapy, and its development can be slowed or stopped by discontinuation of therapy and subsequently anticoagulation. Indeed, Guo and colleagues suggested the use of anticoagulant therapy for primary FHN. However, anticoagulants cannot play a protective role in secondary FHN.
![i.php?p=13. Oxigenoterapia hiperbarica]()
It can also result from bleeding, infection, high bone marrow pressure, bone marrow infiltration, and bone marrow edema. Physiologically, as the pressure increases inside the extravascular region, the microcirculation in the vessels that cross the tissue increases. This is not a common occurrence. Often, steroid use influences lipid metabolism. This process will soon lead to fat cell hypertrophy. Subsequently, the intravenous pressure will increase and the ischemic state will appear. Although osteonecrosis is largely associated with hypercholesterolemia and/or hypertriglyceridemia, lipid abnormalities related to osteonecrosis have been well documented in Gaucher disease (GD). Gaucher disease (GD) is a lysosomal storage disorder caused by impaired β-glucocerebrosidase function which results in the accumulation of glucocerebrosides in cells and changes in the ordering of membranes. However, blocking microcirculatory blood flow is not necessarily the initial pathological event. The lysosomal content released from Gaucher cells can damage the vessel's membrane, with localized osteonecrosis extending to the surrounding areas.
- The third pathophysiological mechanism is being investigated: extra-bone venous obstruction. Although extra-bone vein damage occurs, there is still uncertainty as to whether it is a cause or an effect. In addition, it may have limited clinical significance. Recently, Shah et al. reviewed the literature on this topic and investigated increased intraosseous pressure as a pathogenic process in FHN. In particular, interruption of blood flow or venous stasis has been associated with increased pressure in osteonecrotic samples.
Since the 1970s, scientists have studied dysbaric osteonecrosis and explained the radiographic features of this pathology. It is avascular bone necrosis induced by exposure in hyperbaric environments, typical for workers with polluted and compressed air. A review of the literature on dysbaric osteonecrosis has shown that incomplete decompression procedures lead to decreased blood supply and subsequent osteonecrosis; this is due to the entry of nitrogen bubbles into the areas containing the bone marrow.
What are the effects of oxygen therapy on the body?
- Decreases inflammation
- Increases the body's oxygen saturation by 20-30%
- Increases the body's immunity
- Increases blood circulation and stimulates the formation of new capillaries
- Decreases toxins in the body
- Stimulates the production of new blood cells
- Increases healing rate
The therapeutic mechanisms of action of HBO are based on increasing both the partial pressure of inspired O2 and the hydrostatic pressure. The latter mechanism contributes to determining the compression of all regions filled with gas in the body (Boyle's law) and it is essential to allow effective treatment of those conditions in which gas bubbles are present in the body and cause an embolism or intravascular or intra-tissue bubble decompression. However, most patients treated with HBO do not suffer from bubble-induced lesions, benefiting from the other mechanism of HBO therapy: elevated O2 partial pressures. The increased partial pressures of O2, obtained in different tissues, leads to the increase of the production of reactive O2 species (ROS), as well as of the reactive nitrogen species (RNS), the latter being the cause of hyperoxia. Randomized controlled studies have already shown that the clinical efficacy of HBO depends on the modulation of intracellular transduction cascades, leading to the synthesis of growth factors, promoting wound healing, and ameliorating postischemic and post-inflammatory lesions.
The actual inability to determine which will be the correct dose of HBO to administer in each case still depends on the lack of level 1 evidence; in fact, the current scientific literature does not yet allow a clear identification of the optimal treatment protocol.
However, HBO is positioned among the possible and feasible therapies that promise to provide a delay in hip arthroplasty surgery; such therapy may show a beneficial effect without having the invasiveness of a surgical approach.
HBO increases extracellular oxygen concentration and reduces ischemia and cellular edema by inducing vasoconstriction. Studies have already reported radiographic improvement in stage I FHN, according to the Steinberg classification, as well as better pain control. Against the background of the possible effects of HBO, a reduced pressure of the bone marrow is induced, which leads to significant relief of pain and an increased release of oxygen in the ischemic cells, thus ameliorating the crushing syndrome, to prevent a progression in another necrosis, stimulating angiogenesis and oxygenation. It also induces the improvement of osteoclast and osteoblast function for remodeling and repair. Moreover, HBO is also able to stimulate multipotent fibroblasts in the bone marrow with additional help in the process of osteogenesis.
![i.php?p=21. Valoarea terapiei cu oxigen]()
In the treatment of FHN, HBO facilitates oxygenation of hypoxic tissue and reduces edema by creating a high concentration of dissolved oxygen and by inducing vasoconstriction. This may explain the early relief of pain seen in patients treated in this way; by saturating the extracellular fluid with diffuse oxygen, HBO treatment will lead to better oxygenation of ischemic bone cells, independent of circulating hemoglobin and without the need for additional energy to ensure the dissociation of oxygen from hemoglobin. The late effects of HBO are bone resorption, revascularization, and osteogenesis.
Yang et al. quantitatively evaluated hemodynamic flow in animal models with steroid-induced FHN using CT images. Especially in the early stages, they evaluated how HBO therapy led to improved regional blood flow in ischemic tissues. Also, they found high-quality bone regeneration and well-regenerated hematopoietic tissue. Moreover, recent studies focusing on the differentiation of osteoblasts and osteoclasts have shown positive results due to hyperbaric oxygen treatment. In particular, HBO has changed the balance between bone formation and bone resorption, promoting regeneration.
Clinical presentation
Early detection of FHN is crucial because the clinical success of therapy is closely linked to the stage at which treatment has begun. There are several procedures capable of intercepting an FHN suspect at the onset or in the early stages of the disease: currently, histological studies, scintigraphy, functional bone assessment, radiography, magnetic resonance imaging (MRI), and computed tomography (CT) ) are the most current diagnostic methods available. In an early stage, FHN is usually asymptomatic or characterized by mild pain radiating to the knee and/or ipsilateral buttocks.
It can occur with limited hip movement, as well as intense pain, especially during a forced rotation. FHN should be considered if the patient feels pain in the hip and has no risk factors in his medical history. In particular, regular radiographs can determine the early stages of necrosis. Patients with a history of necrosis should be observed for bilateral FHN; this condition was in 70% of cases.
The classification systems currently used for FHN include the Liver and Steinberg systems. Liver classification is based substantially on standard radiographic presentations, where phase I presents normal images; phase II indicates a normal contour, with evidence of bone remodeling; stage III is characterized by collapse or subchondral flattening of the femoral head; and phase IV indicates a narrowing of the joint space, with secondary degenerative changes in the acetabulum. The Liver classification system, however, is based on radiographic images; therefore, the actual size of the lesion cannot be quantified to a more accurate and precise measure of the radiological appearance of the disease.
Steinberg extends the Liver system in six stages, including quantifying the involvement of the femoral head in stages I-VI, with three additional subsets each: mild (less than 15% radiographic involvement of the articular surface of the femoral head), moderate (with 15-15 30% involvement of the articular surface of the femoral head) and severe stages (involvement of more than 30% of the articular surface of the femoral head).
Recently, the Osseous Circulation Research Association (ARCO) recommended a third standardized classification system based on an interpolated comparison of different findings of the procedure: radiography, MRI, bone scan, and histological findings. Even this cannot eliminate operator-dependent intrinsic variability, which makes the Liver and ARCO classification systems not yet reliable enough to assess the occurrence of FHN.
FHN is currently diagnosed by simple anterior and postero-lateral radiographs of the hip, followed by MRI; it is considered the most accurate standard. Other existing tools for assessing FHN presentation, such as venography, bone marrow pressure measurements, and nuclear biopsy, are rarely used.
Clinical management of femoral head necrosis
Many therapeutic modalities have been proposed, and their effects have recently been reviewed by Sen and Zalavras, and Lieberman.
If left untreated, FHN is a progressive disease process in the affected hip that has an intact joint survival rate of less than 60% in 5 years; Also, the stage III survival rate is less than 10%.
Current clinical evidence demonstrates that HBO is capable of prolonging the survival rate of affected hips:
- Reis and colleagues treated 12 patients with stage I ANFH with a daily HBO session for a total of 100 HBO sessions. They reported that 81% of patients exposed to HBO had a normal MRI compared to only 17% in the untreated group.
- A prospective double-blind, randomized, controlled study evaluated hyperbaric oxygen therapy in a cohort of 20 patients with unilateral FHN (stage II liver). All patients were treated with either compressed oxygen or compressed air (HBA); each patient received 30 sessions of HBO or HBA for 6 weeks. After the initial 6-week treatment, all patients with HBA received HBO. From this point on, the study is moving towards an observational design study. Range of motion (ROM), stabilometry, and pain were assessed at the beginning of the study and after 10, 20, and 30 treatments by a physician. MRI was obtained before, at 12 months post-HBO, and after 7 years of follow-up. There was a significant improvement in pain after HBO after an average of 20 treatment sessions. The ROM improved similarly during HBO, for all parameters, after 20-30 treatments. At 7 years, all patients maintained their condition and none required hip arthroplasty; an almost complete radiographic cure of osteonecrosis was observed in seven of the nine hips. Hyperbaric oxygen therapy appears to be a viable treatment in patients with FHN II Liver.
- Koren and colleagues used HBO to treat 68 patients (78 joints) with stage I and II disease; The HBO protocol of these authors involved 100% oxygen breathing at 2.0-2.4 ATA for 90 minutes, for a total of 20 treatment sessions. They reported that 88% of the HBO treatment group had an MRI improvement and a 93% joint survival rate.
- Recently, the long-term effect of HBO in 217 patients with stage I, II, and III ANFH was investigated. These results validated previous findings: HBO can significantly improve the hip condition, alleviate pain, and more importantly, avoid hip surgery in most patients with stage II disease. Moreover, this study further shows the beneficial effects of HBO in stage III patients, where hip pain is significantly reduced in most patients, hip surgery is avoided in about half of patients, and the results are maintained for up to 4 years.
One of the first studies, proposed by Baixe and colleagues, said that 20 HBO treatments were enough to reduce pain. As previously reported, Camporesi and colleagues showed that after 20-30 treatment sessions, patients had substantially improved pain. However, 20 HBO treatments are not enough to completely heal the balance.
Although there is ample evidence of the beneficial effects of HBO, there is still no agreement on the number of HBO treatments required. The recent work of Bosco and colleagues generated an average number of 83.3 ± 24.8, while in the study of Koren et al., The average number of treatments was 78.3 ± 24.2. In other studies, the number of treatments varies between 20 and 120.
A large number of sessions have been shown to be effective in relieving pain and improving mobility and have prevented arthroplasty in approximately 80% of cases. In particular, approximately 90% of Liver I and II patients and half of Liver III patients after HBOT no longer needed surgery and all related complications for at least 4 years.
New perspectives
Despite several clinical trials supporting the benefits of HBOT in patients with osteonecrosis, therapy is still being studied worldwide. This may be due to several factors, including the apparently high number of HBO treatments required, plus a limited amount of clinical evidence for FHN, most of the evidence is based on ex vivo and in vitro studies. Molecular mechanisms responsible for regenerative responses from HBOT are still debatable. Thus, the basic mechanism of action is still unclear.
A recent study investigated the effect of HBO on serum osteoprotegerin (OPG) and/or inhibition of osteoclast activation. Twenty-three patients with unilateral FHN in stage I, II, and III agreed to receive treatment: patients received standard HBOT; 19 patients completed the study. Serum OPG levels were obtained at the beginning of HBOT (T0), after 15 sessions (T1), after 30 sessions (T2), after a break of 30 days (T3), and at the end of treatment, after 60 sessions (T4). . Magnetic resonance imaging (MRI) was obtained at T0 and approximately 1 year after the end of HBO treatments to compare pre-HBOT status with post-HBOT lesion size.
The results were:
- HBOT reduced the symptoms of pain in all patients.
- HBOT significantly reduced the size of the lesion in all patients in stages I and II and in 2 of 11 patients in stage III.
- HBOT increased serum OPG levels, but the kappa-B receptor activator did not change.
This evidence determines the influence of HBO on the immune system and inflammatory processes. Indeed, one of the initial studies by Lukich et al. suggested an immunosuppressive effect of HBO therapy in patients with rheumatoid arthritis. Subsequently, other studies have reinforced these findings. Specifically, the authors showed that inhibition of TNF-alpha and interleukin-1β occurs after HBO therapy for indomethacin-induced enteropathy and in chronic constriction-induced lesion neuropathy. The following are some examples of tissue cytokine changes produced after HBO.
IL-1β is a pro-inflammatory cytokine that responds to lesions or infections by binding to the IL-1 type 1 receptor (IL-1R) to the accessory protein IL-1R [54]. Although it belongs to a class of structurally different cytokines, IL-1 resembles TNF-α. Activation of IL-1 leads to downstream activation of NF-κB and JNK. Fukushima et al. found that IL-1β has a stimulating effect on osteoclast formation through increasing expression of RANKL. IL-1β, like TNF-α and IL-6, is produced by stromal cells and monocytes. These cytokines can synergistically stimulate osteoclast differentiation leading to a net increase in RANKL activity.
IL-6 has been shown to have a double effect on osteoclastic differentiation. During the inflammatory process, monocytes/macrophages produce IL-6, which can directly stimulate pre-osteoclastic cells to differentiate and activate. aLSO, IL-6 can stimulate dental/osteoblastic cells. IL-6 will then promote osteoclastic differentiation. Thus, there is a dual contribution, direct and indirect interaction, in which IL-6 can regulate bone regeneration. In vivo studies for IL-6 found that in transgenic mice with overexpressed IL-6 there are reduced osteoblasts and increased osteoclasts leading to osteopenia. Accordingly, IL-6-deficient mice had reduced osteoclasts and lower levels of bone erosion. Kurokouchi and colleagues discovered the effect of TNF-α to increase the expression of IL-6 and ICAM-1 genes. Therefore, lower TNF-α levels resulting from HBOT exposure could explain the reduction in IL-6. This effect, summing up the synergistic effects of TNF-α, IL-6 and RANKL, could eventually lead to decreased levels of osteoclastogenesis and therefore better patient outcomes.
In the case of FHN, HBOT results in a reduced amount of circulating TNF-α. We propose the following mechanism: HBOT leads to reduced levels of TNF-α, which leads to decreased TNF-α binding to the type 1 p55r receptor and thus decreases the level of NF-κB activation.
Understanding the molecular mechanism of action of HBOT remains the best approach to obtain information about this treatment.
IN CASE YOU HAVEN'T ALREADY HEARD ABOUT US
Centrokinetic is the place where you will find clear answers and solutions for your motricity problems. The clinic is dedicated to osteoarticular diseases and is divided into the following specialized departments:
- Orthopedics , a department composed of an extremely experienced team of orthopedic doctors, led by Dr. Andrei Ioan Bogdan, primary care physician in orthopedics-traumatology, with surgical activity at Medlife Orthopedic Hospital, specialized in sports traumatology and ankle and foot surgery. .
- Pediatric orthopedics , where children's sports conditions are treated (ligament and meniscus injuries), spinal deformities (scoliosis, kyphosis, hyperlordosis) and those of the feet (hallux valgus, hallux rigidus, equine larynx, flat valgus, hollow foot).
- Neurology , which has an ultra-performing department, where consultations, electroencephalograms (EEG) and electromyography (EMG) are performed.
- Medical recovery for adults and children , department specialized in the recovery of performance athletes, in spinal disorders, in the recovery of children with neurological and traumatic diseases. Our experience is extremely rich, treating over 5000 performance athletes.
- Medical imaging , the clinic being equipped with ultrasound and MRI, high-performance devices dedicated to musculoskeletal disorders, and complemented by an experienced team of radiologists: Dr. Sorin Ghiea and Dr. Cosmin Pantu, specialized in musculoskeletal imaging.
Find the latest news by following the Facebook and YouTube accounts of the Centrokinetic clinic.
.jpg)
.jpg)
.jpg)